HPC Solutions in Healthcare: How It’s Accelerating Medical Breakthroughs
High-Performance Computing (HPC) is transforming healthcare by enabling unprecedented computational power for complex medical simulations, genomic analysis, and personalized medicine. As medical research generates exponentially larger datasets and requires increasingly sophisticated modeling, HPC solutions for healthcare have become essential infrastructure for modern medical breakthroughs. This article in MR CFD, explores how advanced computing architectures are accelerating discoveries that were previously impossible, with particular focus on computational fluid dynamics applications using ANSYS Fluent in medical research and clinical applications.
Ready to Accelerate Medical Breakthroughs with ANSYS HPC?
You’ve seen how High-Performance Computing is driving the future of healthcare, enabling complex simulations and analyses previously out of reach. If your work in medical research, device development, or clinical applications relies on ANSYS Fluent or other ANSYS solvers, leveraging this power is no longer optional – it’s essential for accelerating discovery. Don’t let computational bottlenecks impede your progress. Our ANSYS HPC service offers seamless, on-demand access to computing resources specifically optimized for ANSYS software, perfectly suited for the demanding simulations required in healthcare.
Experience the difference true HPC makes: complete complex medical simulations in hours instead of days. This dramatic speedup accelerates your research cycles, allows for more intricate and patient-specific modeling, and significantly boosts your productivity in a field where time is critical. Access the high-performance computing power needed to push the boundaries of medical science with ANSYS, without the overhead of managing complex infrastructure.
Explore HPC for Faster ANSYS Solves
The Evolution of Healthcare Computing: From Mainframes to Exascale
The journey of computing in healthcare represents one of the most profound technological transformations in modern medicine. What began with simple electronic record-keeping has evolved into computational systems capable of modeling the human body at the molecular level and processing vast datasets to uncover patterns invisible to human researchers.
In the 1950s and 1960s, early mainframe computers first entered medical institutions primarily for administrative tasks and basic data management. These systems, though revolutionary for their time, offered computational power measured in kiloflops (thousands of floating-point operations per second)—barely sufficient for even the most basic medical calculations. The 1970s saw the emergence of minicomputers in research laboratories, enabling the first computational biology applications, though still severely limited by processing capabilities. By the 1980s, the introduction of parallel computing architectures began to hint at the potential for more complex medical simulations, with systems reaching megaflop performance (millions of operations per second).
The true transformation began in the 1990s with the emergence of cluster computing, where multiple computers were networked together to tackle larger problems collectively. This period marked the first genuine HPC in healthcare applications, enabling more sophisticated genomic analysis and the earliest attempts at molecular modeling for drug discovery. Performance benchmarks during this era show a dramatic acceleration:
| Era | Computing Paradigm | Typical Performance | Example Healthcare Application |
| 1960s | Mainframes | Kiloflops | Patient records, basic statistics |
| 1980s | Early parallel systems | Megaflops | Basic molecular modeling |
| 1990s | First clusters | Gigaflops | Initial genomic sequence alignment |
| 2000s | Modern HPC clusters | Teraflops | Protein folding, medical imaging |
| 2010s | Petascale systems | Petaflops | Whole genome analysis, complex simulations |
| 2020s | Exascale computing | Exaflops | Digital twins, real-time personalized medicine |
The early 2000s brought teraflop (trillions of operations per second) computing to medical research, coinciding with the completion of the Human Genome Project—a 13-year effort that modern HPC systems could now complete in days. This era saw the first applications of computational fluid dynamics in cardiovascular research, though simulations remained simplified and computationally expensive.
The last decade has witnessed the emergence of petascale computing (quadrillions of operations per second), enabling unprecedented applications in medical research:
- Complete patient-specific cardiovascular modeling
- Virtual clinical trials for medical devices
- Real-time processing of complex diagnostic imaging
- Simulation-based surgical planning
Today, as we enter the exascale era (quintillions of operations per second), we stand at the threshold of capabilities that will fundamentally transform medicine. These systems can simultaneously model multiple physiological systems, incorporate genetic information into treatment planning, and enable real-time analysis of population-level health data during pandemic response.
The impact of this computational evolution on medical breakthroughs cannot be overstated. Treatments that once took decades to develop can now be designed in years or months. Diagnostic capabilities that required invasive procedures can now be simulated non-invasively. And personalized medicine—tailored to an individual’s unique genetic and physiological characteristics—has moved from theoretical concept to clinical reality.
Understanding HPC Architecture in Modern Medical Research
Modern medical computing infrastructure represents a complex integration of specialized hardware, software, and networking components specifically optimized for healthcare’s unique computational challenges. Understanding these architectures is essential for researchers and healthcare organizations seeking to leverage HPC effectively.
At the foundation of any medical HPC system are the compute nodes—the workhorses that execute the complex calculations required for medical simulations and data analysis. Unlike general-purpose computing, medical HPC demands specialized processor architectures optimized for the specific mathematical operations common in healthcare applications. Modern systems typically employ a heterogeneous computing approach, combining different processor types to maximize performance across varied workloads:
- CPU (Central Processing Units): Provide broad computational capability with high clock speeds and sophisticated instruction sets, ideal for sequential code execution and overall system management. Medical applications typically benefit from high core-count CPUs with large cache sizes to handle complex algorithms.
- GPU (Graphics Processing Units): Deliver massive parallelism with thousands of simpler cores, perfectly suited for the matrix operations common in medical imaging, molecular dynamics, and fluid simulations. NVIDIA’s A100 and AMD’s Instinct MI250 accelerators have become staples in medical HPC, offering 5-20× performance improvements for key healthcare algorithms compared to CPU-only implementations.
- FPGA (Field Programmable Gate Arrays): Provide reconfigurable hardware acceleration for specialized algorithms, particularly beneficial for real-time processing of medical sensor data and custom genomic sequence alignment.
The interconnect fabric binding these components represents another critical architectural element. Medical simulations often require extensive communication between compute nodes, making interconnect bandwidth and latency key performance determinants:
| Technology | Bandwidth | Latency | Suitability |
| InfiniBand HDR | 200 Gbps | 0.5-0.7 μs | Excellent for CFD, genomics |
| Intel Omni-Path | 100 Gbps | 0.8-1.0 μs | Good for general medical HPC |
| Ethernet (100G) | 100 Gbps | 1.5-2.0 μs | Suitable for distributed analytics |
Storage architecture for medical HPC presents unique challenges due to the massive datasets involved. A typical genomic sequencing operation can generate terabytes of data, while medical imaging archives grow by petabytes annually. Modern medical HPC employs multi-tier storage architectures:
- High-Performance Parallel File Systems (like Lustre or BeeGFS) providing hundreds of GB/s throughput for active computation
- Flash-based intermediate storage for frequently accessed datasets and intermediate results
- Object storage systems for long-term retention of medical data with appropriate compliance capabilities
Healthcare workloads demand specific architectural optimizations that differentiate medical HPC from other scientific computing domains:
- Memory subsystems with higher capacity and bandwidth to accommodate the large biological datasets
- I/O optimization for the continuous streaming of patient monitoring data or medical imaging
- Specialized accelerators for specific medical algorithms like genomic alignment or heart model simulation
in HPC for ANSYS Fluent applications in healthcare, architectural considerations become even more specialized. Computational fluid dynamics simulations of blood flow or respiratory systems require:
- High memory bandwidth to handle the complex mesh representations of anatomical structures
- Enhanced floating-point precision for accurate representation of biological fluid properties
- Low-latency node interconnects to manage the tightly-coupled nature of CFD calculations
- Optimized I/O subsystems for handling the large mesh files and simulation results
The architectural requirements scale dramatically with simulation complexity. A simplified 2D blood flow simulation might run on a workstation, while a fully-coupled 3D simulation of a complete cardiovascular system with fluid-structure interaction requires a true HPC cluster with hundreds or thousands of cores.
| Simulation Type | Computational Requirements | Storage Requirements | Typical Infrastructure |
| Basic 2D CFD | 16-32 cores | 10-50 GB | Workstation |
| 3D Steady-State | 64-256 cores | 100-500 GB | Small cluster |
| 3D Transient | 256-1024 cores | 1-5 TB | Medium cluster |
| Multi-physics FSI | 1000+ cores | 5-20 TB | Large HPC system |
| Population-scale studies | 10,000+ cores | 100+ TB | Supercomputer |
Understanding these architectural considerations is crucial for healthcare organizations planning HPC investments. The right architecture can mean the difference between simulations that take weeks versus hours, or analyses that capture critical medical insights versus those that miss subtle patterns in the data.
Genomic Sequencing: How HPC Reduced Analysis Time from Years to Hours
The genomic revolution represents one of the most dramatic examples of how HPC in healthcare has transformed medical research capabilities. The computational demands of genomic analysis have driven some of the most significant advances in high-performance computing architecture, while simultaneously, HPC breakthroughs have enabled entirely new approaches to genomic medicine.
When the Human Genome Project completed its first draft in 2000 after 13 years of international effort, the computational resources required were staggering for the time—yet modest by today’s standards. The project utilized what would now be considered entry-level HPC systems, with the final assembly computations running on systems with just gigaflops of performance. The cost: approximately $3 billion. Today, a complete human genome can be sequenced and analyzed in under 24 hours for less than $1,000, representing a performance improvement of over 100,000× in just two decades.
This transformation has been driven by three parallel developments:
- Algorithmic innovations that dramatically reduced computational complexity
- HPC architecture advancements specifically optimized for genomic workloads
- Specialized hardware accelerators designed for sequence alignment and variant calling
The computational pipeline for modern genomic analysis illustrates the scale of this HPC challenge:
- Raw Data Processing: Convert sequencer output to readable sequences → 1-2 TB of raw data per human genome → Highly parallelizable across thousands of cores
- Sequence Alignment: Map fragments to reference genome → Computationally intensive pattern matching → Benefits from specialized accelerators (GPUs, FPGAs) → Requires high memory bandwidth
- Variant Calling: Identify differences from reference genome → Statistical analysis across aligned sequences → Memory-intensive operations → Benefits from high core counts with large caches
- Clinical Interpretation: Determine medical significance → Knowledge-based analysis requiring database access → Machine learning integration for pattern recognition → Benefits from heterogeneous computing architectures
The performance evolution of these pipelines demonstrates the impact of HPC advancements:
| Era | System Capabilities | Genome Analysis Time | Throughput |
| 2000 | Early clusters (Gigaflops) | Years | 1 genome/year |
| 2010 | HPC clusters (Teraflops) | Weeks | 50 genomes/year |
| 2015 | GPU-accelerated (100s of Teraflops) | Days | 1000 genomes/year |
| 2020 | Specialized HPC (Petaflops) | Hours | 10,000+ genomes/year |
| 2025 (projected) | Exascale systems | Minutes | 1,000,000+ genomes/year |
This computational acceleration has enabled entirely new medical applications that were previously inconceivable:
- Rapid pathogen genomics during disease outbreaks, allowing strain identification and tracking in real-time during epidemics
- Cancer genomics that can sequence tumor DNA during surgery, providing oncologists with mutation information before the patient leaves the operating room
- Pharmacogenomics that predicts medication responses based on a patient’s genetic profile, enabling truly personalized treatment plans
- Rare disease diagnosis through whole genome sequencing, ending diagnostic odysseys for patients with previously unidentifiable conditions
The technical implementations powering these advances leverage specialized HPC architectures. For example, the Edico Genome DRAGEN platform uses FPGA-based acceleration to achieve a 30× speedup for genome analysis compared to traditional CPU implementations. Similarly, NVIDIA’s Clara Parabricks leverages GPU acceleration to reduce analysis time from 30 hours to under 1 hour for a 30× whole genome.
The computational requirements for population-scale genomics—analyzing millions of genomes to identify patterns across populations—have pushed the boundaries of HPC even further. Projects like the UK Biobank, which aims to sequence 500,000 genomes, require exascale computing capabilities and novel approaches to distributed computing and data management.
The storage and data management challenges are equally significant. A single human genome generates approximately:
- 100-200 GB of raw sequencing data
- 30-50 GB of aligned sequence data
- 1-5 GB of variant data
For population-scale projects, this translates to exabytes of data that must be stored, managed, and analyzed—requiring specialized HPC storage architectures with hierarchical data management capabilities.
The future of genomic HPC lies in real-time analysis capabilities that will enable:
- Continuous monitoring of pathogen evolution during outbreaks
- Immediate genomic analysis in emergency medicine
- Integration of genomic data with other clinical information for comprehensive health modeling
These advances demonstrate how HPC has not merely accelerated existing genomic workflows but has fundamentally transformed what’s possible in genomic medicine—creating capabilities that simply could not exist without massive computational resources.
Digital Twins and Patient-Specific Modeling with ANSYS Fluent
The concept of digital twins—virtual replicas of physical entities that simulate real-world behaviors—represents one of the most promising applications of HPC in healthcare. When applied to patient-specific modeling, this approach enables unprecedented precision in treatment planning and medical device design. ANSYS Fluent, with its advanced computational fluid dynamics capabilities, has emerged as a critical tool in this revolution, particularly for cardiovascular, respiratory, and neurological applications.
Patient-specific modeling fundamentally transforms the traditional “one-size-fits-all” approach to medicine. By creating detailed computational models based on an individual patient’s anatomy and physiology, clinicians can simulate interventions before performing them, predict outcomes with greater accuracy, and optimize treatments for each unique patient. This paradigm shift has been made possible by the convergence of three technologies:
- Advanced medical imaging (CT, MRI) providing high-resolution anatomical data
- Sophisticated computational fluid dynamics software like ANSYS Fluent
- High-performance computing infrastructure capable of running complex simulations in clinically relevant timeframes
The workflow for creating patient-specific models using ANSYS Fluent involves several computationally intensive steps:
- Image Acquisition & Segmentation: Convert medical imaging (CT/MRI) to 3D anatomical models, using semi-automated segmentation with machine learning assistance, outputting an accurate 3D representation of patient anatomy.
- Mesh Generation: Create computational mesh representing the fluid domain, requiring high-resolution near boundaries (vessel walls), typically 5-50 million elements for accurate cardiovascular models.
- Boundary Condition Assignment: Apply patient-specific flow conditions from clinical measurements, incorporate tissue properties and physiological parameters, and define simulation parameters based on clinical objectives.
- Parallel Simulation Execution: Distribute computation across HPC resources, solve Navier-Stokes equations with appropriate turbulence models, and capture transient phenomena across multiple cardiac cycles.
- Post-Processing & Clinical Interpretation: Extract clinically relevant parameters (pressure gradients, wall shear stress), visualize results for clinical decision-making, and compare intervention scenarios for optimal treatment selection.
The computational demands of these simulations are substantial. A typical patient-specific cardiovascular simulation in ANSYS Fluent requires:
| Simulation Aspect | Typical Requirements | Clinical Impact |
| Mesh Resolution | 10-50 million elements | Accuracy of flow prediction near vessel walls |
| Time Steps | 1000+ per cardiac cycle | Capture of transient flow phenomena |
| Simulation Duration | 3-5 cardiac cycles | Establishment of periodic solution |
| Compute Resources | 256-1024 cores | Delivery of results within clinical timeframes |
| Storage Requirements | 1-5 TB | Preservation of full solution for future analysis |
Real-world applications of patient-specific modeling with ANSYS Fluent have demonstrated significant clinical value:
Cardiovascular Applications
In cardiovascular medicine, ANSYS Fluent simulations enable detailed analysis of blood flow patterns in complex anatomies. For patients with aortic aneurysms, these simulations can predict rupture risk with greater accuracy than traditional diameter-based assessments. Studies have shown that incorporating wall shear stress predictions from CFD simulations improves risk stratification by 30-40% compared to conventional methods.
For surgical planning, virtual testing of different intervention options has proven invaluable. In complex congenital heart defect repairs, surgeons can evaluate multiple surgical approaches virtually before entering the operating room. One study at Boston Children’s Hospital demonstrated that pre-surgical CFD modeling changed the planned surgical approach in 30% of complex cases, leading to improved outcomes.
Respiratory Applications
In pulmonary medicine, ANSYS Fluent enables detailed modeling of airflow in the bronchial tree, helping predict drug delivery patterns for inhaled medications or optimizing ventilator settings for critically ill patients. During the COVID-19 pandemic, these capabilities proved particularly valuable, with researchers using HPC-powered Fluent simulations to:
- Optimize ventilator designs for emergency production
- Model aerosol transmission in hospital environments
- Predict the effectiveness of various mask designs
These simulations typically require even higher mesh resolutions than cardiovascular models due to the complex branching structure of the airways, with element counts often exceeding 100 million for detailed respiratory models.
Neurological Applications
Cerebrovascular modeling represents another frontier for patient-specific simulation. For patients with intracranial aneurysms, ANSYS Fluent simulations can predict flow patterns that correlate with rupture risk. Similarly, for stroke patients, virtual testing of thrombectomy devices can help optimize device selection and procedural approaches.
The computational requirements for these neurological applications are particularly demanding due to the need for:
- Extremely fine mesh resolution to capture small vessels
- Complex rheological models for blood behavior in low-flow conditions
- Fluid-structure interaction to model vessel wall deformation
The clinical impact of these patient-specific models extends beyond individual treatment planning. The aggregation of simulation results across patient populations is creating valuable databases that inform medical device design, surgical technique development, and clinical guideline formulation. As HPC resources become more accessible and simulation workflows more automated, patient-specific modeling is transitioning from a research tool to a standard component of clinical decision-making.
ANSYS Fluent’s HPC Requirements for Advanced Cardiovascular Simulations
Cardiovascular simulations represent some of the most computationally demanding applications in medical computing, requiring specialized HPC configurations to deliver clinically relevant results within practical timeframes. ANSYS Fluent, as an industry-leading CFD solver, has specific hardware and software requirements to efficiently handle these complex biomedical simulations.
The computational challenges of cardiovascular CFD stem from several factors that distinguish these simulations from traditional engineering applications:
- Geometric complexity: Vascular structures feature intricate branching patterns, curvature, and patient-specific anatomical variations that necessitate high-resolution meshes
- Multi-physics coupling: Blood flow simulations often require fluid-structure interaction to model vessel wall deformation and tissue response
- Non-Newtonian fluid behavior: Blood exhibits complex rheological properties that require sophisticated material models
- Pulsatile flow conditions: Cardiac-driven flow creates transient conditions requiring fine temporal resolution
- Multi-scale phenomena: Critical flow features span multiple scales from millimeters (large vessels) to micrometers (near-wall regions)
These challenges translate into specific HPC requirements for ANSYS Fluent to deliver accurate, timely results for cardiovascular applications:
Processor Architecture Requirements
ANSYS Fluent performance for cardiovascular simulations scales differently across processor architectures. Benchmark testing reveals significant performance variations:
| Architecture | Relative Performance | Optimal Use Case |
| Intel Xeon Gold | Baseline (1.0×) | General-purpose simulations |
| AMD EPYC Milan | 1.2-1.4× | Memory-intensive large meshes |
| Intel Xeon Ice Lake | 1.3-1.5× | Balanced performance |
| AMD EPYC Genoa | 1.4-1.6× | High core-count scaling |
| NVIDIA A100 GPU | 2.0-3.0× (with GPU solver) | Accelerated steady-state solutions |
For optimal performance, cardiovascular simulations benefit from:
- High core count processors (32+ cores per socket)
- Large L3 cache (64MB+) to accommodate complex solver data
- High memory bandwidth (200+ GB/s per socket)
- AVX-512 or equivalent vector extensions for floating-point operations
Memory Requirements
Memory consumption represents a critical constraint for cardiovascular simulations. The relationship between mesh size and memory requirements follows predictable patterns:
| Mesh Size (Elements) | Minimum RAM Required | Recommended RAM | Simulation Type |
| 1-5 million | 16-32 GB | 64 GB | Simplified steady-state |
| 5-20 million | 64-128 GB | 256 GB | Standard pulsatile flow |
| 20-50 million | 256-512 GB | 1 TB | Detailed FSI models |
| 50-100 million | 1-2 TB | 4 TB | Multi-vessel systems |
| 100+ million | 4+ TB | 8+ TB | Whole-circulation models |
Memory bandwidth becomes particularly important for transient simulations where solution data must be transferred between memory and processors at each time step. Systems with high memory bandwidth (200+ GB/s per socket) demonstrate 20-40% performance improvements for cardiovascular simulations compared to systems with standard memory configurations.
Storage Architecture
Cardiovascular simulations generate massive datasets that require specialized storage solutions:
| Workflow Phase | I/O Pattern | Throughput Requirement | Capacity Requirement |
| Mesh Loading | Sequential Read | 2-5 GB/s | 10-100 GB per case |
| Solution Progress | Random Write | 1-3 GB/s | 100-500 GB per case |
| Results Storage | Sequential Write | 5-10 GB/s | 1-5 TB per case |
| Post-processing | Random Read | 3-8 GB/s | Varies by analysis |
For production environments running multiple cardiovascular simulations, a multi-tier storage architecture is recommended:
- High-performance parallel file system (Lustre, BeeGFS) for active simulations
- Flash storage tier for frequently accessed patient data and results
- Object storage for long-term archival of simulation results
- Automated data lifecycle management to migrate results between tiers
Interconnect Requirements
The tightly-coupled nature of CFD calculations makes interconnect performance critical for scaling cardiovascular simulations across multiple nodes:
| Interconnect Technology | Latency | Bandwidth | Scaling Efficiency at 1024 Cores |
| 100 Gb Ethernet | 1.5-2.0 μs | 12.5 GB/s | 40-60% |
| InfiniBand HDR | 0.5-0.7 μs | 25 GB/s | 70-85% |
| InfiniBand NDR | 0.4-0.5 μs | 50 GB/s | 80-90% |
| Proprietary (Slingshot, OmniPath) | 0.5-0.8 μs | 25-32 GB/s | 75-85% |
For cardiovascular simulations with complex geometries, the communication overhead increases substantially as the simulation scales across nodes. Testing shows that latency-sensitive operations in the pressure-velocity coupling algorithm benefit significantly from high-performance interconnects, with scaling efficiency dropping below 50% on standard Ethernet networks beyond 512 cores.
Software Optimization
Maximizing ANSYS Fluent performance for cardiovascular simulations requires specific software configurations:
| Setting | Recommendation | Performance Impact |
| Solver Type | Pressure-based coupled | 30-40% faster than segregated |
| AMG Solver Settings | F-cycle, aggressive | 15-25% convergence improvement |
| Parallel Partitioning | METIS with load balancing | 10-20% better scaling |
| Precision | Double (required) | Necessary for accuracy |
| Turbulence Model | k-ω SST or LES | Application-dependent |
| Discretization | Second-order upwind | Required for accuracy |
Additional software considerations include:
- Proper MPI implementation selection (Intel MPI, OpenMPI, or MVAPICH2)
- Processor affinity settings to optimize NUMA access patterns
- I/O configuration to leverage parallel file systems effectively
- Use of in-situ visualization to reduce storage requirements
Scaling Characteristics
Understanding how cardiovascular simulations scale is essential for HPC resource planning. Benchmark data shows distinctive scaling patterns, with ideal scaling being linear, while actual scaling efficiency decreases as the number of cores increases beyond a certain point.
Typical parallel efficiency for medical simulations:
- 90-95% efficiency up to 128 cores
- 80-90% efficiency from 128-512 cores
- 70-80% efficiency from 512-2048 cores
- 50-70% efficiency beyond 2048 cores
The optimal core count depends on simulation size and time constraints:
| Simulation Size | Optimal Core Count | Time to Solution | Parallel Efficiency |
| 5-10M elements | 64-128 | 2-4 hours | 85-95% |
| 10-50M elements | 256-512 | 4-8 hours | 75-85% |
| 50-100M elements | 512-1024 | 8-12 hours | 65-75% |
| 100M+ elements | 1024-4096 | 12-24 hours | 50-65% |
For most clinical applications, configuring systems to deliver results within 12-24 hours represents the optimal balance between computational resource utilization and clinical workflow integration. This typically requires 256-1024 cores for standard cardiovascular models, though complex multi-physics simulations may require significantly more.
The specialized HPC requirements for ANSYS Fluent in cardiovascular applications highlight the importance of purpose-built computing infrastructure for advanced medical simulations. As these simulations become increasingly integrated into clinical workflows, optimizing HPC configurations becomes essential for delivering actionable results within timeframes that impact patient care.
Accelerating Drug Discovery: HPC’s Role in Pharmaceutical Breakthroughs
The pharmaceutical industry has undergone a computational revolution, with HPC solutions for healthcare dramatically transforming the drug discovery process. Traditional drug development—a process that historically took 10-15 years and cost billions of dollars—is being compressed through computational methods that enable researchers to screen millions of compounds, simulate molecular interactions, and predict drug efficacy with unprecedented accuracy.
The impact of HPC on pharmaceutical research can be measured in both time and cost savings. Recent studies indicate that computational methods reduce early-stage drug discovery timelines by 40-50% and cut associated costs by 25-30%. More importantly, HPC-driven approaches increase the probability of clinical success by identifying potential failures earlier in the development pipeline.
Molecular Dynamics Simulations: The Computational Foundation
At the heart of computational drug discovery are molecular dynamics (MD) simulations—computationally intensive calculations that model the physical movements and interactions of atoms and molecules. These simulations reveal crucial insights about protein-ligand binding, conformational changes, and drug mechanism of action that would be impossible to observe through experimental methods alone.
The computational requirements for these simulations are staggering:
| System Size | Atoms | Simulation Time | Computational Demand |
| Small Protein | 10K-50K | Nanoseconds | 100s of core-hours |
| Protein-Ligand | 50K-100K | Microseconds | 1000s of core-hours |
| Membrane Protein | 100K-500K | Microseconds | 10,000s of core-hours |
| Cellular System | 1M-10M | Milliseconds | Millions of core-hours |
Modern drug discovery leverages specialized MD software optimized for HPC environments, including:
- AMBER (Assisted Model Building with Energy Refinement)
- GROMACS (GROningen MAchine for Chemical Simulations)
- NAMD (NAnoscale Molecular Dynamics)
- Desmond (part of Schrödinger’s platform)
These packages have been extensively optimized for parallel execution, with performance scaling demonstrated across thousands of cores. GPU acceleration has proven particularly effective for MD simulations, with NVIDIA’s specialized hardware delivering 10-30× performance improvements compared to CPU-only implementations.
Virtual Screening: Searching Chemical Space at Scale
Virtual screening represents another computationally intensive phase of modern drug discovery, where millions of compounds are evaluated for potential binding affinity to target proteins. This approach dramatically reduces the number of compounds that need to be synthesized and tested experimentally.
HPC enables two complementary approaches to virtual screening:
- Structure-based virtual screening: Docking simulations that predict how compounds bind to protein targets
- Ligand-based virtual screening: Machine learning models that identify patterns in known active compounds
The computational demands scale with the size of the chemical libraries being screened:
| Library Size | Compounds | CPU Core-Hours | GPU-Accelerated Hours | Typical HPC Configuration |
| Focused | 10K-100K | 1,000-10,000 | 100-1,000 | 64-128 cores or 4-8 GPUs |
| Corporate | 1M-10M | 100,000-1,000,000 | 10,000-100,000 | 1,000+ cores or 64+ GPUs |
| Ultra-large | 100M-1B | 10M-100M | 1M-10M | Supercomputing facility |
Recent breakthroughs in ultra-large virtual screening have been enabled by specialized HPC infrastructures. For example, researchers at the University of California used the Summit supercomputer to screen 1 billion compounds against COVID-19 targets in just 24 hours—a task that would have taken years on traditional computing resources.
De Novo Drug Design: Computational Creativity
Perhaps the most advanced application of HPC in drug discovery is de novo drug design—using computational methods to create entirely new molecular structures optimized for specific targets. These approaches leverage generative models, evolutionary algorithms, and reinforcement learning to explore chemical space far beyond known compounds.
The computational architecture for de novo drug design typically involves:
- Target Characterization: Protein structure preparation and binding site analysis, and MD simulations to identify dynamic binding pockets. Requires hundreds to thousands of core-hours per target.
- Generative Model Training: Deep learning on chemical databases (often 100M+ compounds), model optimization and validation. Requires GPU clusters with 16-64 GPUs for days/weeks.
- Compound Generation: Sampling from trained models with target constraints, property prediction and filtering. Moderate parallelization across tens to hundreds of cores.
- Candidate Evaluation: Docking and scoring of generated compounds, and MD simulation of promising candidates. Highly parallelizable across thousands of cores.
- Experimental Validation Planning: Synthesis pathway prediction and ADMET property prediction. Moderate computational requirements.
Recent successes in this field include the development of novel antibiotics against resistant bacteria and the creation of selective kinase inhibitors for cancer treatment—both achieved through HPC-powered computational design methods that identified molecules human researchers would likely never have conceived.
Real-World Impact: Case Studies
The pharmaceutical industry has seen numerous examples where HPC has directly enabled major breakthroughs:
- Case Study 1: COVID-19 Antiviral Development. When the COVID-19 pandemic emerged, researchers leveraged HPC resources to rapidly identify potential treatments. Using a combination of virtual screening and MD simulations, scientists identified several promising compounds within weeks rather than years. The development of Pfizer’s Paxlovid (nirmatrelvir) benefited significantly from computational methods, with HPC simulations helping optimize the molecule’s interaction with the viral main protease.
- Case Study 2: Cancer Immunotherapy Target Discovery. Researchers at a major pharmaceutical company employed HPC-powered simulations to understand the binding mechanism between PD-1 and PD-L1—key proteins in cancer immunotherapy. These simulations, running on a 10,000-core cluster, revealed previously unknown binding dynamics that led to the development of small-molecule inhibitors with improved efficacy and reduced side effects.
- Case Study 3: Alzheimer’s Drug Development. The complex pathology of Alzheimer’s disease has made traditional drug development particularly challenging. HPC-enabled simulations of amyloid-beta aggregation—running on specialized Anton supercomputers—provided unprecedented insights into the molecular mechanisms of disease progression. These simulations guided the design of compounds that specifically target the early stages of protein misfolding, representing a novel therapeutic approach.
Future Directions: Exascale Impact
As exascale computing becomes available to pharmaceutical research, several transformative capabilities are emerging:
- Whole-cell simulations that model entire cellular environments, capturing drug effects across multiple pathways simultaneously
- Patient-specific drug response prediction by incorporating genomic data into pharmacological models
- Real-time adaptive drug design where AI algorithms continuously refine molecular structures based on simulation results
These capabilities promise to further compress drug discovery timelines while increasing success rates—potentially reducing the average time from target identification to clinical candidate from years to months for certain drug classes.
The integration of HPC into pharmaceutical research represents one of the most significant technological transformations in modern medicine, enabling researchers to explore chemical space and biological interactions with unprecedented depth and efficiency. As computational methods become more sophisticated and HPC resources more powerful, we can expect an acceleration in the pace of drug discovery that will directly translate to improved patient outcomes across a wide range of diseases.
Medical Imaging Revolution: How HPC Powers AI-Enhanced Diagnostics
Medical imaging has undergone a profound transformation through the integration of high-performance computing and artificial intelligence, creating diagnostic capabilities that were unimaginable just a decade ago. This convergence of HPC in healthcare with advanced imaging algorithms has not only enhanced the quality and speed of traditional diagnostics but has enabled entirely new approaches to disease detection, characterization, and monitoring.
The computational demands of modern medical imaging are extraordinary, driven by increasing resolution, dimensionality, and complexity. A typical hospital now generates petabytes of imaging data annually—from traditional modalities like CT, MRI, and ultrasound to advanced techniques like functional MRI, spectroscopic imaging, and molecular imaging. Processing this data at scale requires specialized HPC infrastructure optimized for both traditional image processing and emerging AI-based analysis.
Computational Challenges in Advanced Medical Imaging
Modern medical imaging presents unique computational challenges that distinguish it from other HPC workloads:
- Data Volume: High-resolution 3D and 4D imaging studies routinely generate gigabytes of data per patient examination
- Real-time Requirements: Many clinical workflows require immediate processing and analysis
- Complex Algorithms: Advanced reconstruction and analysis techniques involve computationally intensive operations
- Heterogeneous Workloads: Imaging pipelines combine different computational patterns (signal processing, linear algebra, neural network inference)
These challenges translate into specific HPC requirements:
| Modality | Data Size | Processing Type | HPC Requirement |
| CT Reconstruction | 1-5 GB | FFT-based, iterative | GPU acceleration |
| MRI Reconstruction | 2-10 GB | Complex matrix ops | High memory bandwidth |
| fMRI Analysis | 5-20 GB | Statistical, ML | High core count + GPU |
| 3D Ultrasound | 1-3 GB | Real-time processing | Low-latency inference |
| Digital Pathology | 10-100 GB | CNN-based analysis | GPU clusters |
| Molecular Imaging | 1-5 GB | Iterative recon | GPU acceleration |
For a typical hospital imaging department, the aggregate computational requirements are substantial:
| Workflow Component | Daily Processing Volume | Computational Demand | Storage Requirement |
| Image Acquisition | 100-500 studies | 10-50 TFLOPS | 1-5 TB/day |
| Image Reconstruction | 100-500 studies | 50-200 TFLOPS | Temporary |
| Primary Analysis | 100-500 studies | 100-500 TFLOPS | 5-10 TB/day |
| AI-based Detection | 50-250 studies | 200-1000 TFLOPS | Metadata only |
| Advanced Visualization | 20-100 studies | 50-200 TFLOPS | Temporary |
| Research Applications | 5-20 studies | 100-500 TFLOPS | 1-2 TB/day |
AI-Enhanced Imaging: The Computational Foundation
The integration of artificial intelligence into medical imaging has dramatically increased computational requirements while simultaneously delivering unprecedented diagnostic capabilities. Modern AI-enhanced imaging leverages several deep learning architectures:
- Convolutional Neural Networks (CNNs) for feature detection and classification
- U-Net and V-Net architectures for semantic segmentation of anatomical structures
- Generative Adversarial Networks (GANs) for image enhancement and synthesis
- Transformer models for contextual understanding of medical images
Training a state-of-the-art medical imaging AI model typically requires:
- 8-64 high-end GPUs (NVIDIA A100 or equivalent)
- 100-1000 GB of high-speed memory
- Weeks of continuous computation
- Petaflops of aggregate computing power
Once trained, the deployment of these models presents different computational challenges. While inference requires less computation than training, the real-time requirements of clinical workflows necessitate optimized hardware and software configurations:
| AI Application | Inference Time Requirement | Typical Hardware | Optimization Techniques |
| Emergency Triage | <30 seconds | Edge GPU (A10, T4) | Model quantization, TensorRT |
| Routine Screening | <5 minutes | Workstation GPU | Batch processing, pipeline parallelism |
| Complex Analysis | <30 minutes | Small GPU cluster | Model ensemble, multi-stage pipeline |
| Research Applications | Hours/days | HPC cluster | Full precision, exhaustive analysis |
Clinical Applications and Computational Requirements
The computational requirements vary significantly across different clinical applications:
- Diagnostic Radiology
In diagnostic radiology, AI algorithms assist radiologists by automatically detecting abnormalities, quantifying disease burden, and prioritizing worklists. These applications typically process 3D volumes (CT/MRI) or 2D images (X-ray) and must deliver results within minutes to maintain clinical workflow efficiency.
Computational requirements for a typical radiology AI deployment include:
- 4-8 NVIDIA T4 or A10 GPUs for inference
- 64-128 GB system memory
- High-speed storage (NVMe) for image caching
- Network connectivity to PACS (Picture Archiving and Communication System)
- Digital Pathology
Digital pathology represents one of the most data-intensive medical imaging applications. A single whole-slide image can contain 100,000 × 100,000 pixels (10 gigapixels), requiring specialized processing techniques:
- Tile Extraction: Divide gigapixel image into manageable tiles (typically 256×256 pixels), parallelize across multiple CPU cores.
- Feature Extraction: Process each tile through CNN backbone (ResNet, EfficientNet), distribute across multiple GPUs.
- Context Integration: Combine tile-level features with spatial context, memory-intensive operations requiring high-bandwidth interconnects.
- Classification/Segmentation: Final diagnostic analysis based on integrated features, often requires ensemble of models for optimal accuracy.
This pipeline requires specialized HPC configurations:
- High core-count CPUs for tile processing
- Multiple GPUs for parallel inference
- Large system memory (256GB+) for holding whole-slide representations
- High-bandwidth storage for rapid image access
- Functional and Molecular Imaging
Advanced techniques like functional MRI, PET-CT, and molecular imaging generate multi-dimensional datasets that capture physiological processes over time. Analysis of these datasets requires both traditional signal processing and modern deep learning approaches:
- Signal denoising and artifact removal
- Motion correction across temporal sequences
- Pharmacokinetic modeling of contrast agent or tracer dynamics
- Integration of multi-modal information
These applications benefit from heterogeneous computing architectures that combine:
- GPUs for deep learning components
- High core-count CPUs for statistical analysis
- Large memory capacity for multi-dimensional data manipulation
- Image-Guided Interventions
Perhaps the most demanding in terms of real-time requirements, image-guided interventions require immediate processing of intraoperative imaging to guide surgical decision-making. These applications must deliver sub-second response times while maintaining high accuracy:
| Intervention Type | Imaging Modality | Processing Requirement | Latency Constraint |
| Neurosurgery | Intraoperative MRI | Real-time segmentation | <500 ms |
| Cardiac Procedures | Fluoroscopy/Echo | Motion tracking, enhancement | <100 ms |
| Radiation Therapy | Cone-beam CT | Registration, dose calculation | <1 second |
| Robotic Surgery | Stereoscopic video | Instrument tracking, tissue classification | <50 ms |
Meeting these requirements necessitates specialized edge computing solutions with:
- Dedicated GPUs physically located in or near operating rooms
- Optimized inference engines (TensorRT, OpenVINO)
- Hardware-accelerated image processing pipelines
- Redundant systems for clinical reliability
Infrastructure for Enterprise Medical Imaging AI
Healthcare enterprises implementing comprehensive imaging AI solutions require a multi-tier HPC infrastructure:
- Tier 1: Edge Computing: Located near imaging devices, optimized for low-latency inference, typically 1-2 GPUs per device, handles urgent/emergency workflows.
- Tier 2: Departmental Computing: Centralized within radiology/pathology departments, balanced for throughput and response time, typically 8-16 GPUs in small clusters, handles routine clinical workflows.
- Tier 3: Enterprise Computing: Centralized data center or private cloud, optimized for throughput and scalability, typically 32-128 GPUs in managed clusters, handles batch processing and research applications.
- Tier 4: Cloud/Hybrid Resources: Public cloud or specialized HPC facilities, used for training and research, elastic scaling based on demand, handles periodic intensive computation.
This tiered approach allows healthcare organizations to balance performance requirements against infrastructure costs, deploying appropriate computational resources where they deliver the greatest clinical value.
The revolution in medical imaging powered by HPC and AI continues to accelerate, with each advance in computational capability enabling new diagnostic possibilities. As these technologies mature, we can expect increasingly sophisticated applications that not only detect disease earlier and more accurately but begin to predict disease progression and treatment response—fundamentally transforming the practice of medicine through computational innovation.
HPC Solutions for Healthcare: Building the Optimal Infrastructure
Creating effective HPC solutions for healthcare requires a specialized approach that balances performance, reliability, compliance, and cost-effectiveness. Healthcare organizations face unique challenges when implementing high-performance computing infrastructure, from handling protected health information to integrating with clinical workflows. This section explores the key considerations and best practices for building HPC environments specifically optimized for healthcare applications.
Architectural Considerations for Healthcare HPC
The foundation of any effective healthcare HPC implementation begins with a well-designed architecture that addresses the specific requirements of medical workloads. Unlike general-purpose scientific computing, healthcare HPC must accommodate several distinct characteristics:
- Workload diversity: From genomic analysis to medical imaging to computational fluid dynamics
- Data sensitivity: Protected health information requiring stringent security controls
- Reliability requirements: Clinical applications with minimal tolerance for downtime
- Integration needs: Connections to electronic health records and clinical systems
- Regulatory compliance: HIPAA, GDPR, and other healthcare-specific regulations
These requirements translate into specific architectural patterns involving Computation Clusters, Secure Data Access, Data Management Layers, Visualization Farms, Accelerator Farms, and Storage Infrastructure, all integrated with Clinical Systems.
Each component of this architecture must be designed with healthcare-specific considerations:
- Computation Cluster: The core HPC environment must support diverse workloads with varying computational profiles:
| Workload Type | Optimal Node Configuration | Interconnect Requirement | Typical Scale |
| Genomic Analysis | High core count, high memory | Moderate bandwidth | 100s-1000s of cores |
| Medical Imaging AI | GPU-accelerated, high memory | High bandwidth | 10s-100s of GPUs |
| CFD Simulations | Balanced CPU/memory, high clock | Low latency | 100s-1000s of cores |
| Population Health | High I/O, moderate compute | Storage-optimized | 10s-100s of nodes |
- Accelerator Farm: Specialized hardware for specific healthcare workloads:
- GPU clusters for deep learning and image processing
- FPGA arrays for genomic sequence alignment
- Quantum computing resources for molecular modeling (emerging)
- Data Management Layer: Specialized systems for handling healthcare data:
- De-identification services for PHI protection
- Data lineage tracking for regulatory compliance
- Metadata management for clinical context preservation
- Automated data lifecycle policies for retention requirements
- Storage Infrastructure: Multi-tier systems optimized for healthcare data characteristics:
- High-performance scratch storage for active computations
- Secure object storage for long-term data retention
- WORM (Write Once Read Many) archives for compliance
- Encrypted data protection at rest and in transit
- Clinical Systems Integration: Secure interfaces to healthcare IT:
- HL7/FHIR integration for clinical data exchange
- DICOM connectivity for medical imaging
- Secure API gateways with access controls
- Audit logging for compliance reporting
- Visualization Farm: Resources for interpreting complex results:
- Remote visualization nodes for 3D medical rendering
- Collaborative visualization environments for clinical teams
- Secure thin clients for accessing results from clinical areas
Hardware Selection and Optimization
Selecting appropriate hardware for healthcare HPC requires balancing performance, reliability, and total cost of ownership:
Compute Node Configurations
For general-purpose healthcare HPC nodes, balanced configurations typically deliver the best results:
- CPU: Dual socket, 48-64 cores per socket (AMD EPYC or Intel Xeon)
- Memory: 512GB-2TB DDR5, optimized for bandwidth
- Local Storage: 2-4TB NVMe for job staging
- Network: 200Gbps (HDR InfiniBand or equivalent)
- Reliability Features: ECC memory, redundant power
- Management: Out-of-band management with security features
For specialized workloads, optimized configurations may be required:
- Genomic Analysis Nodes:
- Higher memory-to-core ratio (8-16GB per core)
- Optimized for single-threaded performance
- Large local scratch space for intermediate files
- Medical Imaging Nodes:
- GPU acceleration (4-8 NVIDIA A100/H100 or equivalent)
- High memory bandwidth
- NVLink or equivalent for GPU-to-GPU communication
- CFD Simulation Nodes:
- High clock speed processors
- Low-latency network fabric
- Balanced memory-to-compute ratio
Storage System Design
Healthcare HPC storage requires particular attention to performance, scalability, and data protection:
A comprehensive healthcare HPC storage architecture typically includes:
- High-Performance Tier:
- Parallel file system (Lustre, BeeGFS, or GPFS)
- All-flash or hybrid storage for active datasets
- 10-100 GB/s aggregate throughput
- Sized for 10-20% of total data volume
- Capacity Tier:
- Software-defined storage with erasure coding
- Hybrid flash/disk configuration
- 1-10 GB/s aggregate throughput
- Sized for 30-40% of total data volume
- Archive Tier:
- Object storage with S3-compatible interface
- WORM capability for compliance
- Automated tiering to tape or cloud
- Sized for 50-60% of total data volume
Network Architecture
Network design for healthcare HPC requires careful attention to both performance and security:
- Data Center Fabric:
- Non-blocking topology for predictable performance
- 100/200/400 Gbps interconnects for node-to-node traffic
- Separate control and data planes for security
- Security Segmentation:
- Microsegmentation between security domains
- Data flow controls based on data classification
- Encryption for data in transit
- External Connectivity:
- Secure research network connections (Internet2, NRENs)
- Dedicated clinical network interfaces with strict access controls
- Cloud connectivity for hybrid operations
Software Stack and Environment
The software environment for healthcare HPC requires specialized components beyond traditional scientific computing stacks. This includes Domain-Specific Applications, Healthcare-Specific Middleware, Scientific Computing Stack components, a Security and Compliance Layer, and an Operating System / Hypervisor with healthcare-specific hardening.
Key Software Components:
- Resource Management and Scheduling:
- Workload managers with healthcare-specific policies
- Fair-share scheduling with clinical priority overrides
- Resource reservation for urgent clinical needs
- Container Orchestration:
- Secure container runtime with image verification
- Healthcare-specific container registries
- Compliance-validated application containers
- Data Management:
- Automated PHI detection and protection
- Provenance tracking for regulatory compliance
- Secure multi-tenant data access controls
- Middleware Services:
- Clinical data integration adapters
- Secure API gateways
- Workflow orchestration with compliance checkpoints
- Monitoring and Management:
- Comprehensive audit logging
- Performance monitoring with healthcare-specific metrics
- Automated compliance reporting
Compliance and Security Considerations
Healthcare HPC environments must address stringent regulatory requirements while maintaining performance:
HIPAA Compliance:
| Requirement | HPC Implementation Challenges | Compliance Strategies |
| Access Controls | Multi-user HPC environments with shared resources | Role-based access control, multi-factor authentication, privileged access management |
| Audit Controls | High-volume system logs across distributed infrastructure | Centralized logging, AI-assisted anomaly detection, immutable audit trails |
| Integrity Controls | Ensuring data integrity across parallel file systems | Checksums, digital signatures, blockchain for provenance tracking |
| Transmission Security | Data movement across high-speed interconnects | Encryption for data in transit, secure fabric isolation, network segmentation |
| Device/Media Controls | Large-scale storage systems with frequent hardware rotation | Secure decommissioning procedures, self-encrypting drives, media tracking |
International Regulatory Considerations:
For global healthcare organizations or international research collaborations, additional regulatory frameworks must be considered:
- GDPR (General Data Protection Regulation):
- More stringent consent requirements than HIPAA
- Explicit right to erasure (“right to be forgotten”)
- Restrictions on automated decision-making
- Data transfer limitations outside the EU
- Country-Specific Healthcare Regulations:
- Canada’s PIPEDA and provincial health information acts
- Australia’s Privacy Act and My Health Records Act
- Japan’s Act on the Protection of Personal Information
- China’s Personal Information Protection Law
These international regulations often impose additional requirements for data localization, consent management, and algorithmic transparency that must be incorporated into HPC architectures.
Research-Specific Compliance:
Medical research utilizing HPC introduces additional regulatory considerations:
- IRB (Institutional Review Board) Requirements:
- Documented data protection procedures
- Consent tracking and management
- Protocol adherence monitoring
- Reporting mechanisms for adverse events
- FDA Regulations for Computational Modeling:
- Validation and verification documentation
- Software development life cycle evidence
- Quality system regulations for medical devices
- Good Clinical Practice (GCP) alignment
- 21 CFR Part 11 for Electronic Records:
- Electronic signature requirements
- Audit trail maintenance
- System validation documentation
- Procedural controls and training
Implementing these requirements in HPC environments requires specialized documentation and process controls that must be integrated into the computational workflow.
Security Architecture for Healthcare HPC
Beyond regulatory compliance, healthcare HPC environments require robust security architectures designed to protect sensitive medical data while enabling high-performance computing:
Data Protection Strategies:
Protecting healthcare data in HPC environments requires a multi-layered approach:
- Data Classification and Handling:
- Automated PHI detection and tagging
- Data sensitivity labeling (public, internal, confidential, restricted)
- Policy-based controls for different data classes
- Data lineage tracking throughout computational pipelines
- Encryption Implementation:
- Storage encryption with minimal performance impact
- Memory encryption for sensitive workloads
- Network encryption for data in transit
- Computation on encrypted data (where feasible)
- De-identification Techniques:
- Pseudonymization for linkable research datasets
- K-anonymity and differential privacy approaches
- Synthetic data generation for algorithm development
- Federated computation across protected data silos
Infrastructure Security:
Securing the HPC infrastructure itself presents unique challenges in healthcare environments:
- Secure Compute Environment:
- Hardened node images with minimal attack surface
- Secure boot and trusted execution
- Container security for isolated workloads
- Job segregation based on data sensitivity
- Network Security:
- Microsegmentation of HPC fabric
- East-west traffic monitoring and filtering
- Data flow controls based on sensitivity
- Secure research network connections
- Authentication and Authorization:
- Multi-factor authentication for all access
- Fine-grained authorization for data and resources
- Just-in-time privilege elevation
- Federated identity for research collaboration
Threat Monitoring and Response:
Healthcare HPC environments face sophisticated threats that require advanced monitoring and response capabilities:
- Behavioral Analytics:
- Baseline modeling of normal HPC usage patterns
- Anomaly detection for unusual job characteristics
- User behavior analytics for insider threat detection
- Resource utilization monitoring for cryptojacking
- Threat Intelligence Integration:
- Healthcare-specific threat feeds
- Research institution targeting information
- Vulnerability management for HPC components
- Emerging threat awareness for novel attack vectors
- Incident Response Planning:
- HPC-specific response procedures
- Forensic readiness for compute nodes
- Containment strategies that preserve research data
- Recovery processes with minimal disruption
Ethical Considerations in Healthcare HPC
Beyond security and compliance, healthcare HPC implementations must address complex ethical considerations:
Algorithmic Bias and Fairness:
As HPC enables increasingly sophisticated AI and machine learning in healthcare, addressing algorithmic bias becomes critical:
- Data Representation Issues:
- Underrepresentation of minority populations in training data
- Historical biases encoded in medical records
- Socioeconomic factors influencing data availability
- Geographic disparities in healthcare access
- Fairness Assessment Frameworks:
- Multi-dimensional fairness metrics
- Subgroup performance analysis
- Counterfactual testing methodologies
- Continuous monitoring for emergent bias
- Mitigation Strategies:
- Balanced dataset curation and augmentation
- Fairness constraints in model training
- Post-processing techniques for bias reduction
- Human oversight of algorithmic decisions
Transparency and Explainability:
HPC-powered healthcare applications must balance performance with transparency:
- Explainable AI Approaches:
- Interpretable model architectures where possible
- Post-hoc explanation methods for complex models
- Confidence metrics for clinical decision support
- Uncertainty quantification for risk assessment
- Documentation Requirements:
- Model cards detailing training data and limitations
- Performance characteristics across population subgroups
- Known failure modes and edge cases
- Version control and change management
- Clinical Integration Considerations:
- Appropriate presentation of computational results
- Clear delineation of AI vs. human judgment
- Mechanisms for clinician override
- Continuous performance monitoring
Resource Allocation and Access:
The significant computational requirements of advanced healthcare HPC raise ethical questions about resource allocation:
- Equitable Access Considerations:
- Disparities between well-resourced and underserved institutions
- Potential for “computational divides” in healthcare quality
- Intellectual property barriers to algorithm access
- Commercial vs. public good tensions
- Collaborative Models:
- Shared HPC resources for healthcare research
- Open science initiatives with equitable participation
- Cloud-based democratization of computational capabilities
- Public-private partnerships for infrastructure development
- Sustainability Concerns:
- Energy consumption of large-scale HPC deployments
- Carbon footprint of computational healthcare
- E-waste considerations for hardware lifecycle
- Balancing computational intensity against clinical benefit
Implementation Strategies and Best Practices
Successfully navigating these challenges requires a strategic approach to healthcare HPC implementation:
Governance Frameworks:
Effective governance is essential for balancing innovation with compliance and ethics, involving Executive Oversight, an Ethics Committee, a Compliance Council, and Operational Management.
Key governance components include:
- Data Governance:
- Clear data ownership and stewardship
- Consistent metadata management
- Data quality assurance processes
- Lifecycle management policies
- Algorithm Governance:
- Model development standards
- Validation and verification requirements
- Performance monitoring frameworks
- Update and retirement processes
- Access Governance:
- Resource allocation policies
- Prioritization frameworks for competing needs
- Collaboration agreements and data sharing terms
- External access management
Technical Implementation Approaches:
Several technical approaches can help address healthcare HPC challenges:
- Privacy-Preserving Computation:
- Federated learning across institutions without data sharing
- Homomorphic encryption for computation on encrypted data
- Secure multi-party computation for collaborative analysis
- Trusted execution environments for sensitive workloads
- Compliance Automation:
- Automated PHI detection and protection
- Continuous compliance monitoring
- Audit-ready logging and reporting
- Policy-as-code implementation
- Responsible AI Development:
- Fairness-aware algorithm design
- Explainability by design
- Robust testing across diverse populations
- Continuous monitoring for performance drift
Organizational Strategies:
Beyond technical solutions, organizational approaches are critical:
- Cross-Functional Teams:
- Integration of clinical, technical, and ethical expertise
- Compliance and security representation in project planning
- Patient advocates in governance structures
- Diverse perspectives in algorithm development
- Training and Awareness:
- HPC security training for researchers
- Ethics education for technical teams
- Clinical context for computational specialists
- Leadership awareness of emerging challenges
- Continuous Improvement:
- Regular security assessments and penetration testing
- Compliance program evaluation and updates
- Ethics review of deployed applications
- Feedback loops from clinical implementation
Successfully addressing security, compliance, and ethical challenges in healthcare HPC requires a comprehensive approach that integrates technical solutions with appropriate governance and organizational strategies. By proactively addressing these considerations, healthcare organizations can unlock the transformative potential of high-performance computing while maintaining patient trust and regulatory compliance. As HPC applications in healthcare continue to evolve, these frameworks must adapt to address emerging challenges while enabling the computational innovation that drives medical breakthroughs.
Getting Started with HPC for Healthcare Research: A Practical Guide
Implementing high-performance computing for healthcare research requires careful planning, appropriate resource selection, and effective operational strategies. This practical guide provides healthcare organizations with a structured approach to establishing HPC solutions for healthcare that can accelerate research and enable advanced computational applications.
Assessing Needs and Planning Your HPC Strategy
Before investing in HPC infrastructure or services, healthcare organizations should conduct a thorough assessment of computational needs and develop a comprehensive strategy:
Workload Analysis and Requirements Definition:
Begin by cataloging current and anticipated computational workloads:
- Application Inventory:
- Identify existing computational applications
- Catalog software requirements and dependencies
- Document current performance limitations
- Project future computational needs
- Workload Characterization:
- Analyze computational patterns (CPU, memory, I/O, GPU)
- Determine data volume and growth projections
- Assess security and compliance requirements
- Identify time-sensitivity of results
- User Community Assessment:
- Survey researcher computational needs
- Evaluate technical expertise levels
- Identify collaboration requirements
- Determine support and training needs
This assessment should result in a detailed requirements document that includes:
- Computational Workloads: Application types and computational characteristics, performance requirements (time to solution), scaling requirements (problem sizes, user counts), and software environment needs.
- Data Management Requirements: Data volumes and growth projections, data sensitivity classifications, retention requirements, and sharing and collaboration needs.
- Integration Requirements: Connections to clinical systems, research data pipeline integration, authentication and identity management, and workflow automation needs.
- Compliance Requirements: Regulatory frameworks (HIPAA, GDPR, etc.), institutional policies, audit and reporting needs, and risk management considerations.
- Operational Requirements: Availability expectations, support requirements, training needs, and budget constraints.
Strategic Planning Process:
With requirements defined, develop a comprehensive HPC strategy:
- Vision and Goals Definition:
- Articulate the research vision enabled by HPC
- Define specific, measurable objectives
- Establish key performance indicators
- Align with institutional research priorities
- Deployment Model Selection:
- Evaluate on-premises, cloud, and hybrid options
- Consider total cost of ownership analysis
- Assess organizational capabilities for management
- Determine appropriate scaling approach
- Funding and Sustainability Planning:
- Identify capital and operational funding sources
- Develop cost recovery or chargeback models
- Plan for technology refresh cycles
- Consider grant funding opportunities
- Governance Structure Development:
- Establish oversight committees
- Define resource allocation policies
- Create security and compliance frameworks
- Develop user policies and procedures
Infrastructure Options and Selection
Healthcare organizations have multiple options for accessing HPC resources, each with distinct advantages and considerations:
On-Premises HPC Infrastructure:
Building dedicated HPC infrastructure offers maximum control but requires significant expertise and investment:
- Advantages:
- Complete control over security and compliance
- Optimized for specific healthcare workloads
- No data egress costs or bandwidth limitations
- Potential for lower long-term costs at high utilization
- Considerations:
- Substantial capital investment
- Requires specialized staff for management
- Fixed capacity requires careful planning
- Responsibility for all maintenance and updates
- Best For:
- Organizations with consistent, high-volume workloads
- Environments with strict data sovereignty requirements
- Institutions with existing HPC expertise
- Applications requiring specialized hardware
For organizations pursuing on-premises infrastructure, a reference architecture typically includes Compute Resources (general-purpose, GPU-accelerated, large-memory, visualization), Storage Infrastructure (parallel file system, archive, backup, data transfer), Network Infrastructure (high-speed interconnect, secured research network, DMZ, management network), and Support Infrastructure (monitoring, scheduling, user portal, training).
Cloud-Based HPC Solutions:
Cloud platforms offer flexibility and scalability without capital investment:
- Advantages:
- No upfront capital expenditure
- Elastic scaling to match workload demands
- Access to latest hardware technologies
- Reduced management overhead
- Considerations:
- Potential for higher costs with sustained usage
- Data transfer and storage costs can be significant
- Compliance and security require careful configuration
- Performance may be less predictable
- Best For:
- Organizations with variable or bursty workloads
- Projects with limited duration or funding
- Teams without extensive HPC management expertise
- Applications requiring rapid scaling
Major cloud providers offer healthcare-specific HPC solutions:
| Provider | Healthcare HPC Offerings | Compliance Features | Notable Capabilities |
| AWS | AWS Batch, ParallelCluster | HIPAA BAA, HITRUST | Genomics workflows, medical imaging |
| Microsoft Azure | CycleCloud, Azure Batch | HIPAA BAA, HITRUST | Healthcare APIs, genomics |
| Google Cloud | GCP HPC Toolkit | HIPAA BAA, HITRUST | Healthcare NLP, imaging AI |
| Oracle Cloud | HPC Shapes | HIPAA BAA | Life sciences optimization |
| Specialized Providers | Rescale, Nimbix | Industry-specific compliance | Domain-optimized workflows |
Hybrid and Community Approaches:
Many healthcare organizations benefit from hybrid approaches:
- Hybrid Infrastructure:
- Core on-premises capacity for consistent workloads
- Cloud bursting for peak demands
- Data tiering across environments
- Unified management plane
- Research Computing Consortia:
- Shared infrastructure across institutions
- Pooled expertise and resources
- Collaborative funding models
- Domain-specific optimization
- National Research Platforms:
- Access to national supercomputing resources
- Specialized expertise and support
- Grant-based allocation mechanisms
- Collaboration with computational scientists
Building Your Healthcare HPC Environment
Once you’ve selected an infrastructure approach, several key steps are required to establish an effective healthcare HPC environment:
Software Environment Configuration:
Creating an appropriate software environment is critical for research productivity. A typical healthcare HPC software stack includes System Software (Linux OS, scheduler, monitoring, identity management), Development Tools (compilers, MPI, CUDA/ROCm, languages), Domain-Specific Applications (Genomics, Imaging, Molecular, AI/ML), and Workflow and Reproducibility tools (workflow engines, containers, version control).
Data Management Implementation:
Effective data management is particularly critical for healthcare HPC:
- Data Organization:
- Logical directory structures
- Consistent naming conventions
- Metadata management
- Project organization templates
- Data Protection:
- Access control implementation
- Encryption configuration
- Backup and recovery procedures
- Data integrity verification
- Data Movement and Sharing:
- Secure transfer mechanisms
- Collaboration tools and portals
- External access protocols
- Clinical data integration pipelines
- Data Lifecycle Management:
- Automated tiering policies
- Retention and archiving rules
- Deletion and sanitization procedures
- Audit and compliance reporting
Security Implementation:
Healthcare HPC environments require robust security controls.
User Onboarding and Support:
Effective user support is essential for HPC adoption in healthcare:
- Documentation Development:
- System architecture and capabilities
- Access and usage procedures
- Best practices and optimization guides
- Security and compliance requirements
- Training Program Implementation:
- Basic HPC concepts and usage
- Domain-specific application training
- Advanced optimization techniques
- Security and compliance awareness
- Support Structure Establishment:
- Tiered support model
- Issue tracking and knowledge base
- Office hours and consultation services
- User community and peer support
- Performance Optimization Services:
- Code review and optimization
- Scaling analysis and improvement
- Workflow optimization
- Resource utilization assessment
Operational Best Practices
Maintaining an effective healthcare HPC environment requires ongoing operational excellence:
Monitoring and Management:
Implement comprehensive monitoring for both performance and compliance:
- System Performance Monitoring:
- Resource utilization tracking
- Job performance metrics
- Storage performance and capacity
- Network utilization and latency
- User Activity Monitoring:
- Authentication and access logging
- Data access and movement tracking
- Job submission and execution logging
- Administrative action auditing
- Compliance Monitoring:
- PHI access and handling
- Security control effectiveness
- Configuration drift detection
- Vulnerability management
- Reporting and Analytics:
- Utilization and performance trends
- Resource allocation and fairness
- Cost attribution and chargeback
- Research output metrics
Capacity Planning and Evolution:
Ensure your HPC environment evolves to meet changing research needs:
- Utilization Analysis:
- Resource consumption patterns
- Queue wait times and job characteristics
- Storage growth and access patterns
- User and project growth trends
- Technology Assessment:
- Emerging hardware evaluation
- Software stack modernization
- Architecture optimization
- Cloud integration opportunities
- Refresh Planning:
- Component lifecycle tracking
- Performance/watt improvement assessment
- Capacity expansion planning
- Migration and transition strategies
- Funding and Sustainability:
- Grant opportunities identification
- Cost recovery model refinement
- Collaborative funding approaches
- Return on investment analysis
Research Enablement and Optimization:
Proactively support research excellence through HPC optimization:
- Code Optimization Services:
- Performance profiling and analysis
- Parallelization assistance
- Algorithm optimization
- GPU/accelerator adaptation
- Workflow Optimization:
- Pipeline development assistance
- Automation implementation
- Resource efficiency improvement
- Data management optimization
- Collaboration Facilitation:
- Multi-institutional project support
- Data sharing infrastructure
- Virtual research environments
- Collaborative tool integration
- Research Impact Amplification:
- Computational methods publication support
- Visualization for communication
- Reproducibility enhancement
- Research software preservation
Practical Implementation Roadmap
Implementing HPC for healthcare research typically follows a phased approach:
- Phase 1: Foundation (3-6 months): Complete requirements analysis and strategy development, establish governance structure and policies, implement initial infrastructure (pilot scale), deploy core software environment and security controls, onboard early adopters and validate approach.
- Phase 2: Expansion (6-12 months): Scale infrastructure to production capacity, expand software environment with domain-specific applications, implement comprehensive monitoring and management, develop training program and support structure, integrate with institutional systems and workflows.
- Phase 3: Optimization (12-24 months): Refine resource allocation and scheduling policies, implement advanced data management capabilities, develop specialized application environments, establish performance optimization services, create sustainable funding and growth model.
- Phase 4: Innovation (24+ months): Explore emerging technologies and approaches, develop specialized capabilities for strategic research areas, implement advanced collaboration infrastructure, establish centers of excellence for computational methods, measure and communicate research impact.
Case Example: Medium-Sized Academic Medical Center
To illustrate this approach, consider the implementation journey of a hypothetical academic medical center:
Organization Profile:
- 500-bed teaching hospital
- Medical school with 200 research faculty
- Emerging precision medicine initiative
- Limited existing computational infrastructure
Initial Assessment Findings:
- Growing genomic sequencing generating 5TB monthly
- Medical imaging research requiring GPU computing
- Patient-specific modeling for surgical planning
- Collaborative research with external institutions
Selected Approach:
- Hybrid infrastructure with on-premises core and cloud bursting
- Phased implementation aligned with research priorities
- Shared support model with central IT and research staff
- Governance structure with researcher representation
Implementation Highlights:
- Foundation Phase: Deployed 20-node cluster with 1280 cores and 8 GPUs, implemented 500TB high-performance storage, established secure research network and DMZ, developed HIPAA-compliant security controls, onboarded genomics and imaging research groups.
- Expansion Phase: Doubled compute capacity and added specialized nodes, implemented cloud bursting for peak demands, deployed domain-specific software environments, established formal training and support program, integrated with institutional identity management.
- Optimization Phase: Implemented advanced job scheduling policies, deployed automated data lifecycle management, established performance consulting service, developed chargeback model for sustainability, created research software catalog and repository.
Outcomes and Impact:
- Genomic analysis time reduced from weeks to hours
- Patient-specific surgical modeling implemented in clinical workflow
- Research grant funding increased by 35%
- Computational methods publications increased by 60%
- New multi-institutional collaborations established
This practical guide provides a framework for healthcare organizations to successfully implement HPC solutions that accelerate research and enable advanced computational applications. By following a structured approach to assessment, planning, implementation, and operations, organizations can build effective HPC solutions for healthcare that drive medical innovation while maintaining security, compliance, and operational excellence.
Related Posts
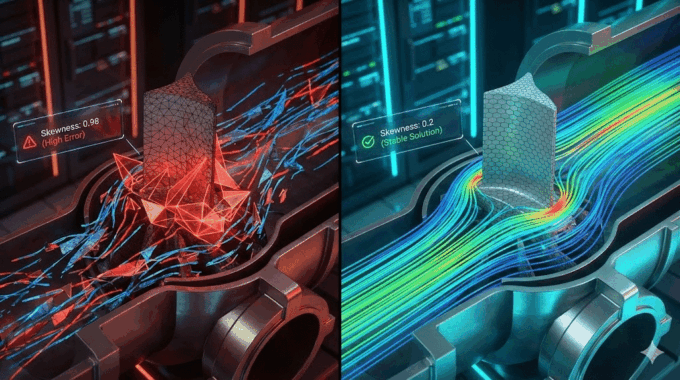
Errors Occurring in Simulations with ANSYS Fluent: A Technical Guide to Convergence & Stability
ANSYS Fluent simulates engineering problems based on the Finite Volume Method (FVM). Consequently, the errors…
How Ansys HPC Servers Accelerate Your Fluent Dynamic Simulations
We have all been there. You hit “Calculate” on a transient simulation, and the estimated…
Ansys HPC Case Study: Accelerating a 120-Million Cell Simulation Using MR CFD’s Ansys HPC Service
In the high-stakes world of aerodynamics, fidelity is everything. But as engineers, we often hit…

Comments (0)